The main aetiological explanation for depression in the public consciousness is undoubtedly the “serotonin hypothesis”. This probably manifests more popularly as the idea that depression is somehow the result of a “chemical imbalance” in the brain, and therefore that sufferers of depression (whose suffering is not in question) are somehow the passive victims of an organic condition, like victims of diabetes, for example, and that this can be righted with medication. It’s a neat explanation, which, I guess, is why it’s so appealing. However, the evidence, as it so often does, suggests that depression is nowhere near this simple.While I agree that the evidence for the serotonin hypothesis of depression (or even the rather wider monoamine hypothesis) is fairly weak, he links to this study finding mixed evidence for an association between suicide, impulsivity, and depression and serotonin metabolite levels. It is worth noting that a review by Mann et al (1989) is often taken as demonstrating that serotonin (or its metabolites) are reduced in the brainstem (source of serotonergic projections in the brain) in suicides, independent of underlying diagnosis. Although this actually only shows reduced serotonin in depressed suicides (if you look at the individual studies) that would actually make it stronger evidence for the hypothesis.
Tuesday 30 March 2010
Serotonin hypothesis of depression
A post from The Twenty-First Floor on the serotonin hypothesis of depression:
Friday 26 March 2010
Treating depression in general medical patients
As a doctor with an interest in psychiatry currently working in general medicine the issue of depression in general medical patients is one that interests me. We commonly see overdoses secondary to depressive illness and depression in patients with terminal diagnoses but also in many other conditions, particularly chronic disease. While we have access to specialist psychiatric or palliative care services for the former conditions that still leaves a substantial number of depressed patients to care for, and that is something of a treatment dilemma.
Physical illness is strongly associated with depression and some 10-20% of general medical inpatients or outpatients have a depressive disorder. This is particularly marked for people with chronic disease where rates range from 11% of diabetics to 20% of people after a heart attack. Depression is a a risk factor for poor prognosis in physical disease, being associated with worse mortality, at least partly mediated via decreased adherence to treatment. Yet evidence shows that physically ill patients receive less antidepressant prescriptions than other depressed patients.
There are some specific challenges in recognising and treating depression in general medicine, early in an admission somatic symptoms of depression can difficult to distinguish from symptoms of physical illness and later on during treatment low mood can be considered 'understandable', with a natural resistance on the part of clinicians to medicalise normal emotional reactions. The inpatient environment is also unusual and stressful and it is unclear whether patients will maintain a low mood or improve when discharged home. Practically, the onset of antidepressants is generally believed to be delayed over two weeks which means that any effect may not be seen during an acute admission and psychological therapies such as CBT are just not available in general medicine.
In recent years the risks of self-harm and discontinuation syndromes with antidepressants have received significant coverage and since Irving Kirsch's 2008 paper much doubt has been raised about overall antidepressant efficacy in any other than the most severe patients. A recent Cochrane Review has addressed the question of antidepressant usage for depression in physically ill patients:
They looked at studies of depression quite broadly defined (major depressive disorder, adjustment disorder, dysthymia) and found 51 studies (mostly in SSRIs but also in tricyclics and a few less common antidepressants), with fluoxetine (Prozac) the drug most commonly studied (12 trials). The physical diseases studied included stroke (11 studies), HIV (7), Parkinson's disease (6), cancer (4), COPD (chronic bronchitis and emphysema; 3), diabetes (3) , heart attacks (2), and renal failure (2). At the two follow-up periods of most interest (6-8 wks and 9-18 wks) there were around 1,000-1,500 subjects included in the analysis.
 Overall they found that antidepressants were similarly effective at all follow-up durations (ranging from 4 to greater than 18 weeks) as seen in the summary figures on the right. We can see an odds ratio of around 2, that is antidepressants roughly double the chance of a 50% improvement in outcome score (most studies used the Hamilton Rating Scale for Depression) or showed a standardised mean difference of around 0.5*
Overall they found that antidepressants were similarly effective at all follow-up durations (ranging from 4 to greater than 18 weeks) as seen in the summary figures on the right. We can see an odds ratio of around 2, that is antidepressants roughly double the chance of a 50% improvement in outcome score (most studies used the Hamilton Rating Scale for Depression) or showed a standardised mean difference of around 0.5*

Looking at other aspects they found that there were more people dropped out of the study from the antidepressant group than the placebo group (this was marginally significant) with an odds-ratio of 1.3 (95% confidence interval 1.0-1.8). Looking at side-effects, dry mouth and sexual dysfunction were both significantly more likely to be reported by those in the antidepressant group, the latter being primarily driven by those taking SSRIs. So overall antidepressants had side-effects sufficiently bad to lead more people to drop out of the study.
The study didn't find any striking differences between the efficacy of SSRIs and other antidepressants, nor differences between taking a narrow (major depressive disorder only) or broad definition of depression.
Looking at the I-squared statistic for trial hetrogeneity we can see that for dichotomous outcomes differences between trials were not very large but for the mean difference outcomes there was very large heterogeneity. However, this seems to be due to two studies with stonkingly big effect sizes (improvements greater than 10 points on the HRSD) and excluding these from analyses drops the I-squared right down without massively affecting the results.
Overall this is quite an interesting finding and it suggests that antidepressants can be really very effective for depression in physically ill patients. But there are some limitations to bear in mind:
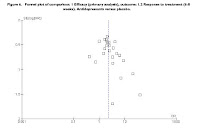 Looking at a funnel plot from the study we can see apparent publication bias (see right), the gap at the bottom left of the pyramid represents missing small trials (or rather, trials with a large standard error) with a large negative effect of antidepressants. This suggests that some negative trials (which we would have predicted would exist based on the effect size we are finding) are missing from the literature included in the review. This is an example of how small positive trials are much more likely to get published than small negative trials which disappear into the file drawer. Publication bias is a known problem in antidepressant trials. When Turner et al analysed data submitted to the FDA before approval** they found that 37/38 positive trials were published but only 14/36 negative trials were published, and 11 of these actually claimed a positive result!
Looking at a funnel plot from the study we can see apparent publication bias (see right), the gap at the bottom left of the pyramid represents missing small trials (or rather, trials with a large standard error) with a large negative effect of antidepressants. This suggests that some negative trials (which we would have predicted would exist based on the effect size we are finding) are missing from the literature included in the review. This is an example of how small positive trials are much more likely to get published than small negative trials which disappear into the file drawer. Publication bias is a known problem in antidepressant trials. When Turner et al analysed data submitted to the FDA before approval** they found that 37/38 positive trials were published but only 14/36 negative trials were published, and 11 of these actually claimed a positive result!
Trial quality was disturbingly low, the authors used the 'Risk of Bias' table from the Cochrane Handbook to score as 'low risk', 'unclear risk', or 'high risk' of bias on six items:
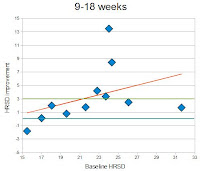
 Only three studies scored as 'low risk' of bias on four or more items*** and only something like 13 on three or more items. The authors find that by looking only at these 13 odd studies the effect size is not grossly different to looking at all the studies. If we just look at the three best quality studies (see right, data from 9-18wks) there is a large effect that is not statistically significant for the mean difference in HRSD scores (but it is significant looking at SMD) that suggests that it isn't purely low quality trials driving the beneficial effect of antidepressants seen in this study.
Only three studies scored as 'low risk' of bias on four or more items*** and only something like 13 on three or more items. The authors find that by looking only at these 13 odd studies the effect size is not grossly different to looking at all the studies. If we just look at the three best quality studies (see right, data from 9-18wks) there is a large effect that is not statistically significant for the mean difference in HRSD scores (but it is significant looking at SMD) that suggests that it isn't purely low quality trials driving the beneficial effect of antidepressants seen in this study.
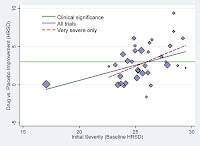 Not looking at the effect of baseline severity in the wake of Kirsch et al and its widespread impact is curious. Kirsch et al, looking at the same FDA data as Turner et al, found that the NICE threshold for 'clinical significance' (an improvement of 3 points on the HRSD or 0.5 SMD) was reached around a baseline severity (as measured by the HRSD) of 26 points, which is classified as 'very severe' by NICE and the American Psychiatric Association (see right). Similar results were found by Fournier et al looking at individual subject level data.
Not looking at the effect of baseline severity in the wake of Kirsch et al and its widespread impact is curious. Kirsch et al, looking at the same FDA data as Turner et al, found that the NICE threshold for 'clinical significance' (an improvement of 3 points on the HRSD or 0.5 SMD) was reached around a baseline severity (as measured by the HRSD) of 26 points, which is classified as 'very severe' by NICE and the American Psychiatric Association (see right). Similar results were found by Fournier et al looking at individual subject level data.
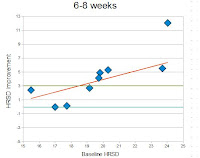 I made a back of the envelope attempt to plot the meta-analysis data against baseline severity**** and we find that the NICE threshold is actually reached at quite low baseline severity (18.5-21.5) which falls in the upper range of moderate through to severe severity.
I made a back of the envelope attempt to plot the meta-analysis data against baseline severity**** and we find that the NICE threshold is actually reached at quite low baseline severity (18.5-21.5) which falls in the upper range of moderate through to severe severity.
 In summary, studies of antidepressant use in physical illness indicate a large effect size that is 'clinically significant' in the 'severe' depression range, and there is a disparity between the large effects sizes in this review and in other studies of depression. Although I have some criticisms of Kirsch et al it seems most likely that this disparity is due to publication bias in the Cochrane meta-analysis. There are some interesting issues regarding the way that studies in general depression usually have a more severe major depression population and any extrapolation to less severe patients is on the basis of few studies whereas the Cochrane review includes a number of less severe conditions and it is possible that this makes it therefore more sensitive to beneficial effects at the lesser degrees of severity. It is also possible that physically ill patients may be more responsive to antidepressants but I'm unconvinced.
In summary, studies of antidepressant use in physical illness indicate a large effect size that is 'clinically significant' in the 'severe' depression range, and there is a disparity between the large effects sizes in this review and in other studies of depression. Although I have some criticisms of Kirsch et al it seems most likely that this disparity is due to publication bias in the Cochrane meta-analysis. There are some interesting issues regarding the way that studies in general depression usually have a more severe major depression population and any extrapolation to less severe patients is on the basis of few studies whereas the Cochrane review includes a number of less severe conditions and it is possible that this makes it therefore more sensitive to beneficial effects at the lesser degrees of severity. It is also possible that physically ill patients may be more responsive to antidepressants but I'm unconvinced.
This study looked at largely outpatient populations with chronic illness and it isn't clear whether the results are directly applicable to inpatient populations but it certainly supports the use of antidepressants in inpatient depression and suggests that at the very least they are likely to be as effective in this population as in the general population of depressed patients.
Finally it is worth noting that NICE has a guideline on treating depression in chronic physical illness which makes recommendations which are broadly similar to those they make for depression in general:
* Standardised mean difference is the difference between the mean outcome scores for the antidepressant and placebo groups divided by the standard deviation, this corresponds to something like a difference of 4 points on the HRSD. Since many studies don't report dichotomous 'improvement' measures, or use different definitions, and these have to be 'imputed' using the mean difference data (making assumptions about how the data is distributed), I prefer mean difference data, ideally using the raw HRSD figures rather than the standardised mean difference (since this can create odd distortions in the data, e.g. in Kirsch et al's study). Almost all studies use the original 17-item HRSD but the few studies that instead use, say, the Montgomery-Åsberg Depression Rating Scale means that the authors have used the SMD so that this data can be combined (the SMD is supposed to allow you to combine data from different scales that are intended to measure the same thing).
** This data should be free from publication bias because the FDA legally mandates the pharmaceutical companies to supply all studies performed on the drug.
*** Cochrane actually discourage adding these up to produce a scale but I can't think of a better way to see which studies are more or less biased.
**** Only including those studies with HRSD data, and those trials where I could access the article and extract it. Since I didn't try too hard to check everything it is quite possible some scoring from scales other than the 17-item HRSD crept in there.
UPDATE
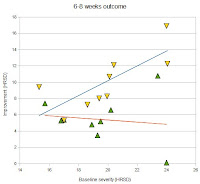 In response to neuroskeptic in the comments, here's the baseline severity data split by antidepressant and placebo groups (as seen in Kirsch et al's analysis), the regression is weighted by sample size, the baseline severity is mean HRSD score, the improvement is mean baseline severity minus mean HRSD score at 6-8 weeks. We can see that increasing baseline severity leads to increasing response to antidepressant with placebo response fairly flat. This was pretty much what we found when we looked at HRSD outcome data from the Kirsch et al study.
In response to neuroskeptic in the comments, here's the baseline severity data split by antidepressant and placebo groups (as seen in Kirsch et al's analysis), the regression is weighted by sample size, the baseline severity is mean HRSD score, the improvement is mean baseline severity minus mean HRSD score at 6-8 weeks. We can see that increasing baseline severity leads to increasing response to antidepressant with placebo response fairly flat. This was pretty much what we found when we looked at HRSD outcome data from the Kirsch et al study.
Physical illness is strongly associated with depression and some 10-20% of general medical inpatients or outpatients have a depressive disorder. This is particularly marked for people with chronic disease where rates range from 11% of diabetics to 20% of people after a heart attack. Depression is a a risk factor for poor prognosis in physical disease, being associated with worse mortality, at least partly mediated via decreased adherence to treatment. Yet evidence shows that physically ill patients receive less antidepressant prescriptions than other depressed patients.
There are some specific challenges in recognising and treating depression in general medicine, early in an admission somatic symptoms of depression can difficult to distinguish from symptoms of physical illness and later on during treatment low mood can be considered 'understandable', with a natural resistance on the part of clinicians to medicalise normal emotional reactions. The inpatient environment is also unusual and stressful and it is unclear whether patients will maintain a low mood or improve when discharged home. Practically, the onset of antidepressants is generally believed to be delayed over two weeks which means that any effect may not be seen during an acute admission and psychological therapies such as CBT are just not available in general medicine.
In recent years the risks of self-harm and discontinuation syndromes with antidepressants have received significant coverage and since Irving Kirsch's 2008 paper much doubt has been raised about overall antidepressant efficacy in any other than the most severe patients. A recent Cochrane Review has addressed the question of antidepressant usage for depression in physically ill patients:
Rayner et al 'Antidepressants for depression in physically ill patients' Cochrane Database of Systematic Reviews 2010, Issue 3.
They looked at studies of depression quite broadly defined (major depressive disorder, adjustment disorder, dysthymia) and found 51 studies (mostly in SSRIs but also in tricyclics and a few less common antidepressants), with fluoxetine (Prozac) the drug most commonly studied (12 trials). The physical diseases studied included stroke (11 studies), HIV (7), Parkinson's disease (6), cancer (4), COPD (chronic bronchitis and emphysema; 3), diabetes (3) , heart attacks (2), and renal failure (2). At the two follow-up periods of most interest (6-8 wks and 9-18 wks) there were around 1,000-1,500 subjects included in the analysis.


Looking at other aspects they found that there were more people dropped out of the study from the antidepressant group than the placebo group (this was marginally significant) with an odds-ratio of 1.3 (95% confidence interval 1.0-1.8). Looking at side-effects, dry mouth and sexual dysfunction were both significantly more likely to be reported by those in the antidepressant group, the latter being primarily driven by those taking SSRIs. So overall antidepressants had side-effects sufficiently bad to lead more people to drop out of the study.
The study didn't find any striking differences between the efficacy of SSRIs and other antidepressants, nor differences between taking a narrow (major depressive disorder only) or broad definition of depression.
Looking at the I-squared statistic for trial hetrogeneity we can see that for dichotomous outcomes differences between trials were not very large but for the mean difference outcomes there was very large heterogeneity. However, this seems to be due to two studies with stonkingly big effect sizes (improvements greater than 10 points on the HRSD) and excluding these from analyses drops the I-squared right down without massively affecting the results.
Overall this is quite an interesting finding and it suggests that antidepressants can be really very effective for depression in physically ill patients. But there are some limitations to bear in mind:
- Most studies were pretty small, almost all with less than 100 subjects and we know that small studies are more likely to overestimate the size of the beneficial effect
- Trial quality was actually pretty low, and low quality trials are known to overestimate effect sizes (more on this below)
- Publication bias was apparent in the studies (more below)
- The effect of baseline severity has become a hot topic since Kirsch et al and this study didn't look at this (more below)
- They looked only at the 10 most common side-effects but not overall adverse event rates, or specifically serious adverse events, and this prevents detection of less common but serious complications (stuff like death or suicide)
- No subgroup analyses were performed to see if antidepressants were more effective in specific physical illnesses (say in stroke rather than HIV)
- They did not look at studies with co-morbid psychiatric illness, this is important because mixed disorders, particularly with aspects of both depression and anxiety, are very common

Trial quality was disturbingly low, the authors used the 'Risk of Bias' table from the Cochrane Handbook to score as 'low risk', 'unclear risk', or 'high risk' of bias on six items:
- Sequence generation
- Allocation concealment
- Blinding
- Incomplete outcome data
- Selective outcome reporting
- Other issues



This study looked at largely outpatient populations with chronic illness and it isn't clear whether the results are directly applicable to inpatient populations but it certainly supports the use of antidepressants in inpatient depression and suggests that at the very least they are likely to be as effective in this population as in the general population of depressed patients.
Finally it is worth noting that NICE has a guideline on treating depression in chronic physical illness which makes recommendations which are broadly similar to those they make for depression in general:
- For low persistent subthreshold depressive symptoms or mild to moderate depression:
- Low intensity psychosocial intervention (e.g. computerised CBT etc.)
- If symptoms persist, previous severe depression, or symptoms compromising care consider either:
- SSRI (citalopram or sertraline first line)
- High intensity psychosocial intervention (e.g. individual CBT etc.)
- Severe depression
- Antidepressant and individual CBT
- Be aware of drug interactions
* Standardised mean difference is the difference between the mean outcome scores for the antidepressant and placebo groups divided by the standard deviation, this corresponds to something like a difference of 4 points on the HRSD. Since many studies don't report dichotomous 'improvement' measures, or use different definitions, and these have to be 'imputed' using the mean difference data (making assumptions about how the data is distributed), I prefer mean difference data, ideally using the raw HRSD figures rather than the standardised mean difference (since this can create odd distortions in the data, e.g. in Kirsch et al's study). Almost all studies use the original 17-item HRSD but the few studies that instead use, say, the Montgomery-Åsberg Depression Rating Scale means that the authors have used the SMD so that this data can be combined (the SMD is supposed to allow you to combine data from different scales that are intended to measure the same thing).
** This data should be free from publication bias because the FDA legally mandates the pharmaceutical companies to supply all studies performed on the drug.
*** Cochrane actually discourage adding these up to produce a scale but I can't think of a better way to see which studies are more or less biased.
**** Only including those studies with HRSD data, and those trials where I could access the article and extract it. Since I didn't try too hard to check everything it is quite possible some scoring from scales other than the 17-item HRSD crept in there.
UPDATE

Saturday 13 March 2010
Summary Care Records
Frontier Psychiatrist has a good post on summary care records, not a fan it appears. I'll share my comments:
I've elected to remain opted in (although I do have a very dull medical history). In my everyday practice on acute medical and surgical takes I have seen many patients who would have benefited from us having access to their SCR - most patients, surprisingly I think, seem to know remarkably little about their past medical history, particularly their surgical history, and in my trust it takes a day or more to get a patient's medical notes (the notes stored for that trust only, anything from elsewhere is very difficult to obtain, including GP data) assuming they haven't been misplaced or lost somewhere on the way. I can think of at least one death in the last few months that might have been avoided if details of past medical history were known.
I have no doubt that, as with many other big government IT projects, there will be massive cost overruns and huge useability issues, but in theory I think it is a good idea.
Popular political science
Interesting piece of popular political science on PoliticalBetting.com:
A new measure by researchers at the University of Manchester shows a significant problem for Gordon Brown: the mood of the country is against Labour on policy competence.
Green and Jennings argue that it is important to study the public mood across a large number of issues: public ratings of party policy competences move together.
This graph shows the authors’ measure, “macro-competence” over six incumbent governments, annually, from 1950 to 2010 (the final data point is February 2010 – the most recently available).
The Tories and medical blogging
It has come to my attention that over the last year or so the Tories have been checking out the medical blogosphere and making discrete contact with influential medical bloggers. I haven't heard of Labour or the Lib Dems making similar overtures. This may reflect the Tories' cutting edge online strategy or just that Labour have completely conceded the ground to them.
What is interesting is the pattern that has seemingly emerged. Rather than outright endorsement of the Tories* there is just explicit condemnation of Labour and what it has done with the NHS. This chimes rather well with the attitude amongst doctors within the NHS. Although naturally leaning towards the Conservatives as upper middle class high earners doctors also have something of an old fashioned public service ethos and are understandably concerned with public service provision (being public sector employees, directly or indirectly, themselves). However, in recent times, after the euphoria of the early years died down, doctors have been fairly vocally critical of Labour's 'reform' agenda, from PFI to patient 'choice'. This is an attitude that you can see daily being expressed by doctors to patients, and this must have a real influence on regular health service users.
But it is only half the story and there is a danger that by failing to spell out what an alternative to Labour's unpopular policies would entail doctors are giving tacit endorsement to the Tories who, in many ways, want to extend and entrench exactly those policies which have proved so unpopular and unsuccesful. I wonder whether the Tories have already figured this out.
* Although perhaps a little nearer the election this will change, with nose peg style 'change' rhetoric.
What is interesting is the pattern that has seemingly emerged. Rather than outright endorsement of the Tories* there is just explicit condemnation of Labour and what it has done with the NHS. This chimes rather well with the attitude amongst doctors within the NHS. Although naturally leaning towards the Conservatives as upper middle class high earners doctors also have something of an old fashioned public service ethos and are understandably concerned with public service provision (being public sector employees, directly or indirectly, themselves). However, in recent times, after the euphoria of the early years died down, doctors have been fairly vocally critical of Labour's 'reform' agenda, from PFI to patient 'choice'. This is an attitude that you can see daily being expressed by doctors to patients, and this must have a real influence on regular health service users.
But it is only half the story and there is a danger that by failing to spell out what an alternative to Labour's unpopular policies would entail doctors are giving tacit endorsement to the Tories who, in many ways, want to extend and entrench exactly those policies which have proved so unpopular and unsuccesful. I wonder whether the Tories have already figured this out.
* Although perhaps a little nearer the election this will change, with nose peg style 'change' rhetoric.
Subscribe to:
Posts (Atom)